Reference Intervals for Common Laboratory Tests
Cesta has a great Statistician and data visualization team. In this blog, we have used National Health and Nutrition Examination Survey (NHANES) 2011-2016 data from the CDC website to showcase our expertise in different Analytical skills.
Introduction
Creating reference intervals (RIs) for clinical lab tests is crucial in healthcare, it helps in disease detection, monitoring, and treatment assessment. These intervals are typically determined using statistical methods based on healthy individuals test results, aiming to cover the range within which most values fall for a given population. This study aimed to investigate racial/ethnic and age differences in RIs of common biochemical and hematological laboratory tests using the National Health and Nutrition Examination Survey (NHANES) 2011-2016, N=4,817 aged 18-40. (Lim et al., 2015) had used NHANES data for 2011-2012, N= 3,077, aged 18-65. We have included additional year's samples for more precise lab ranges.
The process often involves using distribution-based methods like normal or log-normal distributions to establish the 95% confidence intervals or nonparametric percentiles (e.g., 2.5th and 97.5th) from data of healthy subjects.
Despite the recognition of disparities between racial and ethnic groups in RIs for various tests, there's a lack of comprehensive studies comparing RIs among Asians and other racial/ethnic groups in the United States. Asians have often been overlooked due to small sample sizes in studies. NHANES, a significant nationwide survey, historically grouped Asians under "other race" categories until recent years. The inclusion of Asians as a distinct racial/ethnic group in NHANES after 2011-2012 presents an opportunity to investigate whether RIs for common laboratory tests differ among major racial/ethnic groups, including Asians, within a representative sample of healthy US adults.
Methods
Data Source and Study Population: The latest NHANES 2011-2012 data were utilized for this study. NHANES uses a multistage, stratified, cluster sampling design to generate a representative sample of the civilian US population. The data were collected from surveys, examinations, and laboratory tests. A detailed description of survey methods and laboratory and examination data collection procedures is available at the NHANES website (www.cdc.gov/nchs/nhanes.htm).
Race/ethnicity was categorized as non-Hispanic white, non-Hispanic black, Mexican American, other Hispanic, non-Hispanic Asian and other race/ethnicity categories. To compare RIs of laboratory tests in healthy adults by race/ethnicity, only adults aged between 18 and 40 years (inclusive) who rated their overall health status as either “Excellent,” “Very Good,” or “Good”were included. Mexican American and other Hispanic groups were combined into one group for our analysis. Participants who did not specify their race/ethnicity or identified themselves as other mixed race were not included because their sample sizes were too small to produce reliable estimates.
Laboratory Tests: The following 16 biochemical and hematological laboratory tests were examined; albumin, basophils percent, bicarbonate, eosinophils percent, fasting glucose, hemoglobin, lymphocytes percent, mean cell hemoglobin, monocytes percent, platelet count, total bilirubin, total cholesterol, Total calcium, triglyceride, triglycerides, and white blood cell count (WBC). Unadjusted/unweighted upper and lower limits of normal ranges were calculated for the laboratory tests stratified by sex and race/ethnicity(Table 1). The lower and upper limits of the normal range were defined as 2.5th and 97.5th values in percent, respectively. Quantile regression models were conducted for the lower and upper limits of the normal range for each laboratory test comparing across racial/ethnic groups and age group separately for males and females and P values for significance are reported (Table 2). Quantile regression is a robust statistical method that models the shape and location of a distribution since it avoids parametric assumptions about the error distribution. P-value <.05 was considered statistically significant. All analyses were conducted in SAS 9.4 (SAS Institute Inc., Cary, NC).
Results
Table 1 reported Unadjusted/unweighted upper and lower limits of normal ranges for the 16 laboratory tests stratified by sex race/ethnicity (Asian, black, Hispanic, and white) and age group (18-29, 30-40). For comparison, the RIs from the NHANES laboratory manual are also included. Although most normal ranges appeared to be close to the relevant RIs, some normal ranges deviated significantly from the corresponding RIs. For example, the NHANES RIs for Eosinophils percent are 0.7-8.5 % for male and 0.6-7.3 % for female but the normal ranges are 0.6 - 7.7 % for white male, 0.5 - 10.3 % for Black male and 0.4 - 7.0 % for white female. The RIs of Lymphocyte percent is 14.1-47.6 % for female but the normal ranges are 15.4 - 44.7 % for white female and 17.3 - 52.5 % for Black female. The normal range of Triglyceride for Hispanic male was 40 – 527 mg/dL, for white males was 38 – 461 mg/dL, for Black male was 31 – 324 mg/dL Asian male was 44 – 477 mg/dL . The normal range of creatinine for white females was 0.50-1.10 mg/dL but for Asian females was 0.43-0.88 mg/dL.
To address whether these shifts in normal range were statistically significant, quantile regressions were conducted for each parameter separtely for male and female using race/ethnicity and age group as independent variables (Table 2). The P values of each race/ethnicity allowed us to assess whether its normal range is different from black (reference) after adjusting for age group (30-40 reference). All lab parameters showed significant for racial/ethnic or age group difference in either lower or upper percentile. Racial/ethnic differences varied across laboratory tests.
Figure 1(a-e) depicts the variation in the estimated normal ranges by sex and race/ethnicity for the five laboratory tests that showed significant difference bewteen white and black in both percentiles. Significant age group differences were also found in both percentiles in the following laboratory tests: albumin, mean cell hemoglobin, total cholesterol, total calcium, triglyceride, fasting glucose, and triglycerides (Table 2)
Table 1: Normal Ranges of Clinical Laboratory Tests by Sex and Race
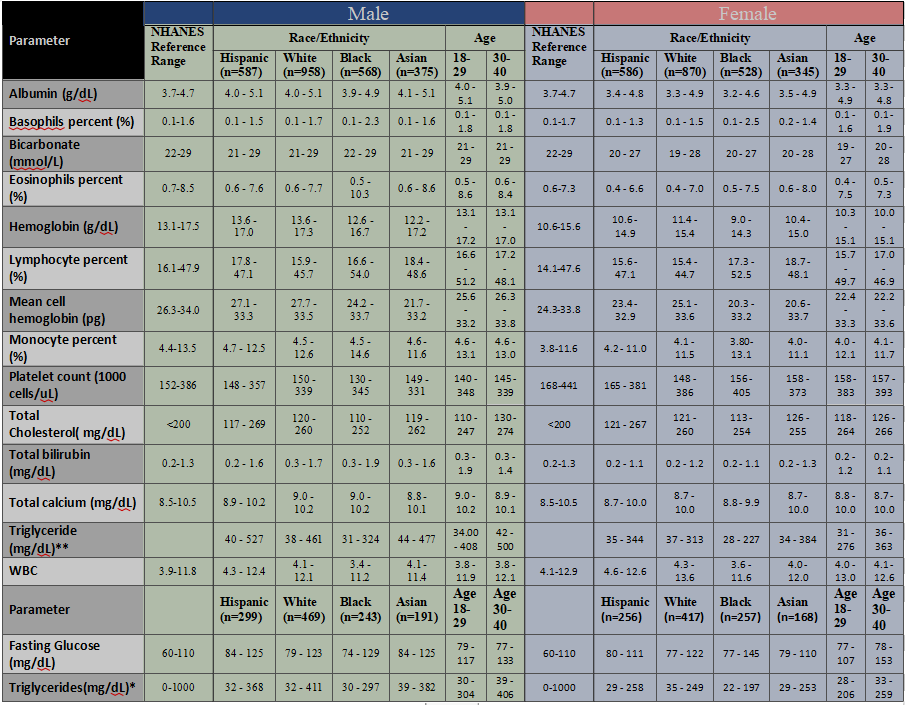
Table 2: Quantile regression P-value for Normal Ranges of Clinical Laboratory Tests for significance of race and age group by Sex
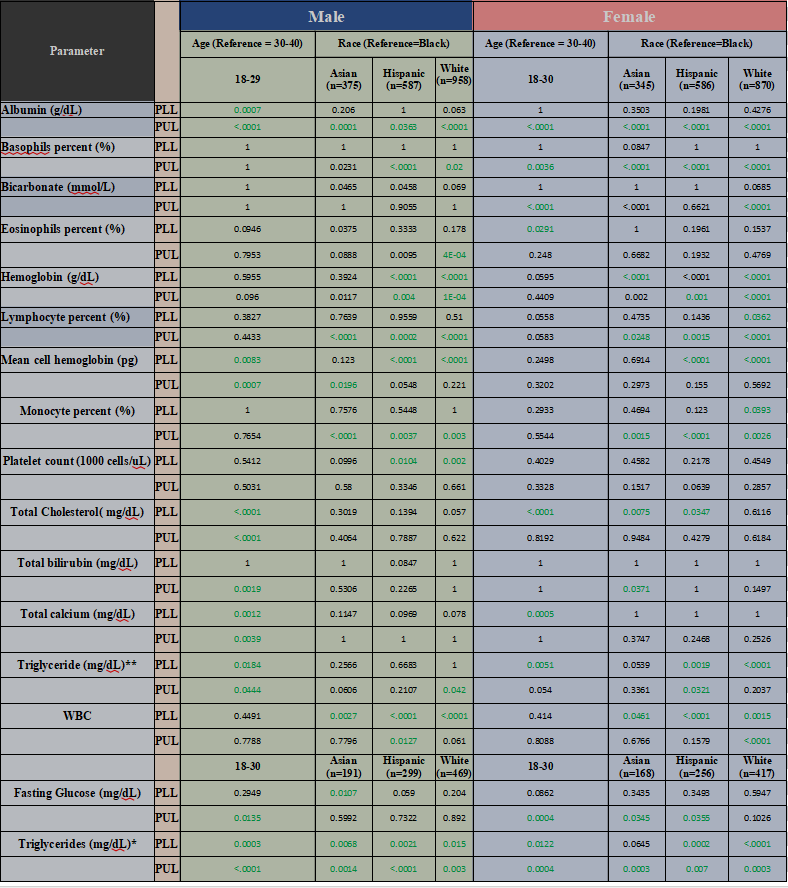
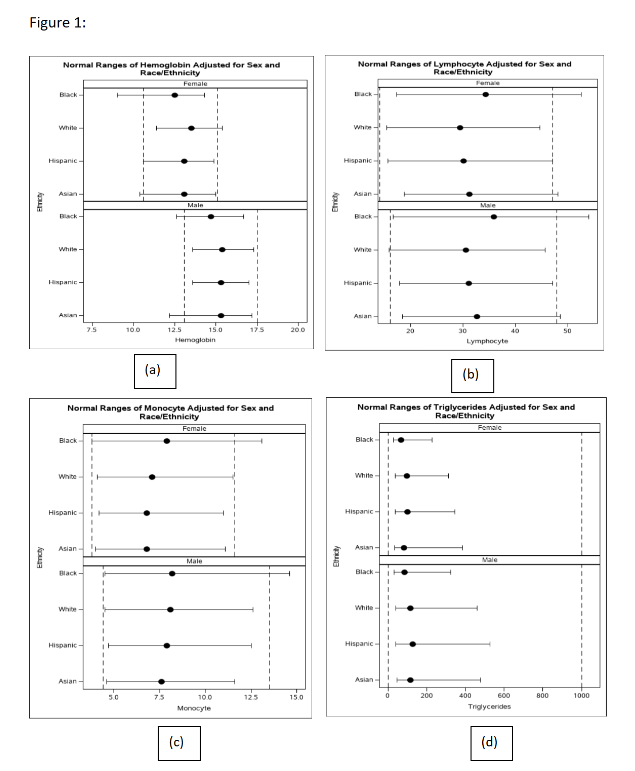
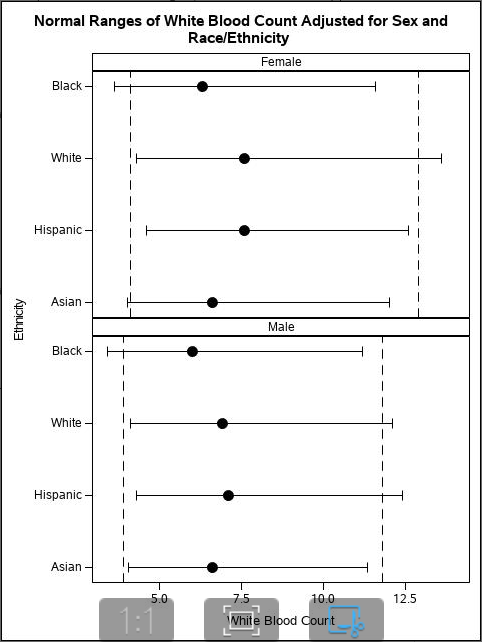
Figure 1: Normal Ranges of Selected Laboratory Tests Adjusted for Sex and Race/Ethnicity. Dashed lines are the reference intervals for each laboratory test based on the NHANES laboratory manual. The horizontal line represents the lower and upper limits of normal range for the subpopulation and the dot on each line represents the estimated median value based on a median analysis. Lower and upper limits of each normal range are the estimated 2.5th and 97.5th values in percent by sex and race/ethnicity, respectively.
These findings highlight the process of developing RIs. Potentially, racial/ethnic-specific RIs will reduce misdiagnosis, over- and under-estimation of disease prevalence rates, the failure or delay in the required reporting of critical laboratory values however, further work is needed to validate these benefits. Physicians and other healthcare providers use the laboratory test results to track clinical outcomes and make clinical decisions to screen asymptomatic people and to identify those at risk and for early detection of diseases. Therefore, accurate RIs for for laboratory tests are important for patients and their caregivers to monitor their health and disease progress. Further work will be necessary to evaluate the impact of using racial/ ethnic-specific RIs to improve health outcomes.
Conclusion
In simpler terms: Different racial and ethnic groups often have different normal ranges for laboratory test results. However, these differences are not usually included in the standard reference intervals (RIs) used by healthcare providers. This lack of specificity can lead to poorer healthcare quality and higher costs. If RIs were adjusted to reflect these differences among racial and ethnic groups, it could improve disease diagnosis, better monitor health, assist in making clinical decisions, and overall enhance healthcare quality.
References
1. Lim E, Miyamura J, Chen JJ. Racial/Ethnic-Specific Reference Intervals for Common Laboratory Tests: A Comparison among Asians, Blacks, Hispanics, and White. Hawaii J Med Public Health. 2015 Sep;74(9):302-10.
2. Cheng CK-W, Chan J, Cembrowski GS, Assendelft OWV. Complete blood count reference interval diagrams derived from NHANES III: stratification by age, sex, and race. Laboratory Hematology. 2004;10(1):42-53
3.Liu X, Liu Y, Tsilimingras D, Campbell KM. Racial disparity in the associations of microalbuminuria and macroalbuminuria with odds of hypertension: results from the NHANES study in the United States. ISRN Hypertension. 2013;2013:8.